
Icaught polio in an epidemic in 1956, when I was six years old. My family lived in a dilapidated country house, Brook Lodge, near the town of Youghal at the mouth of the Blackwater River in County Cork. It was an isolated location: isolated enough for my parents, Claud and Patricia Cockburn, to imagine that we would be safe from the virus that had started circulating in Cork city three months earlier. But our isolation wasn’t complete since my father was travelling to and fro between Cork and London by boat and train. It was a hot summer and my nanny, Kitty Lee, would take me to swim in the sea and build sandcastles on the long sandy beaches. One day in late September, Kitty and I walked into Youghal to visit my cousin Shirley, with whom I often played. She turned out not to be home, but her mother thought I looked feverish and, suspecting that this might be a symptom of polio, drove us back to Brook Lodge in her car.
By the next morning I had a headache and a sore throat. The sheets on my bed were damp with sweat. My mother asked Paddy McMahon, the man who looked after our sheep, horses and vegetable garden, to cycle into Youghal to get a doctor. We lived well enough, like many Anglo-Irish gentry at that time, but our way of life was closer to the 19th than the 20th century and we were often broke. The reason Claud was unwisely travelling to London and back, despite the danger of bringing the infection home, was to boost his earnings from freelance journalism. We didn’t own a car and our telephone had become a casualty of some particularly dire financial emergency.
I was examined by John Gowen, an Englishman with a small practice in Youghal, who drove up to Brook Lodge a couple of hours later. The epidemic had begun in July – polio was sometimes called the ‘summer plague’ – and he can’t have had much doubt about what the diagnosis would be. I liked the cold feel of his stethoscope on my chest and I liked being the centre of attention as he, my mother and Kitty anxiously clustered around my bed. I only became frightened when a cream-coloured ambulance arrived and I was carried downstairs and lifted into the back. ‘The driver will turn on the siren and all the other cars will have to get out of the way,’ my mother said, with forced cheerfulness. The strangeness of it all upset me and I shouted: ‘I don’t want him to sound the horn! I don’t want it!’
The ambulance took me to St Finbarr’s fever hospital, thirty miles away. When I looked at a copy of the hospital register half a century later, it showed that I was admitted on 30 September 1956. Doctors and nurses examined me several times a day, asking me to sit up, move my legs or grip their hands as they tested the damage the virus was doing to my muscles. A cage-like contraption was put on my bed to stop the sheets weighing on my legs. Apart from the medical staff, nobody was allowed to enter the ward and I didn’t see my parents until a nurse came to my bed one day and pointed towards an oval window in the door. On the other side my parents were smiling and waving frantically. I wasn’t entirely separated from my family: my brother Andrew, three years older than me, had been admitted to the hospital a few days after me. He had been called back from his school in Dublin when I was diagnosed and Claud met him at Cork railway station. ‘I really thought that all might be well up to the very last moment when the diesel train pulled into the station and Andrew got out,’ my father recalled. ‘I then saw that his body was bowed slightly forward in an awkward way and he was moving his legs sluggishly.’
The doctors thought Andrew would be crippled more severely than me because he had been diagnosed late: his headmaster must have guessed what was wrong but, presumably because he didn’t want to close the school, chose to put him on a train rather than send him straight to hospital. But Andrew was sent home after three weeks without suffering any long-term physical damage, while I was transferred on 23 October to another hospital, St Mary’s at Gurranabraher, on a hill overlooking Cork city. It had been built as a TB hospital but was rapidly converted for use by the hundreds of polio patients who had survived the fever stage of the illness but were disabled to a greater or lesser degree. Poliomyelitis, to give it its full name, was also called ‘infantile paralysis’: most of the patients were young children, in a state of shock because one or more of their limbs had become floppy and useless.
I hated the place and almost died there. The Irish health authorities had concentrated the best doctors and nurses in St Finbarr’s and let the staff of Gurranabraher, many poorly trained, run it like a barracks, maintaining discipline by threatening the children and shouting. There was an air of violence about the place and, when my parents brought me toys, they were soon broken. I was recovering physically, beginning to take a few faltering steps on wooden crutches with steel callipers on my legs and a rigid plastic waistcoat to support my back. But most of the time I lay on my bed, silent and withdrawn and refusing to eat. Three months in, my parents started to worry that I was giving up on life. ‘He who had been so gay, so alert, inquisitive and talkative,’ my father wrote, ‘seemed to be sinking into a voiceless apathy.’ Deciding that I wouldn’t live long if I stayed there, they asked if there was any medical reason for me not to go home. The doctors believed that I had stopped talking because the virus had damaged my throat muscles and were reluctant to release me, but eventually they relented.
Once I was back in Brook Lodge my morale improved rapidly and so – more slowly – did my physical strength. I had to use a wheelchair at first and couldn’t walk, but I could crawl. My mother was ingenious in coming up with things that I was capable of doing and I painted all the skirting boards in the house. A surgical operation at Whitechapel Hospital in London in 1957 transferred tendons to surviving muscles in my legs and increased my mobility. I gave up the crutches when I was about ten and, although I walked with a severe limp and couldn’t run, I was able to go to school and university and live a fairly normal life.
I was always conscious of being disabled, but for forty years I knew little about the Cork epidemic beyond my own experience. I couldn’t have said with any certainty in what year it had taken place or whether it was caused by a virus or by bacteria. My ignorance was largely self-inflicted: from an early age I sensed that dwelling on what had happened to me, picking at the emotional scar tissue, wasn’t going to do me much good. Only in the late 1990s, when I was in Iraq talking to doctors and patients in ill-equipped hospitals hit by UN sanctions, did I start to feel it strange that I knew more about sickness in Baghdad than I did about polio in Cork, when it had been me lying in a hospital bed.
I started reading about polio, a disease that has probably been around for thousands of years. There is an ancient Egyptian sculpture of a man with a wasted leg, looking very much like my own. Walter Scott was made lame by it as a child. But these were individual cases and it wasn’t until the first half of the 20th century that polio epidemics began to sweep through cities. Before then most people contracted the virus in infancy, when their mother’s antibodies helped them to gain immunity. Long before the Covid-19 pandemic made the phrase ‘herd immunity’ infamous, the pool of people who had polio without knowing it was large enough to prevent epidemics. It was modernity that gave the polio virus its chance: as 19th-century cities acquired clean water supplies and efficient drainage systems, babies were no longer contracting the virus in large enough numbers to provide collective immunity. The most vulnerable populations were in the cities, though some lost protection through geographic isolation: the first epidemic to be scientifically described was on the island of St Helena in 1844, crippling children between the ages of three and five. But polio epidemics hit hardest in New York, Melbourne, Copenhagen, Chicago. Disease in such places was assumed to be associated with poverty, dirt and deprivation, but in fact it was the better off in newly built housing who constituted the majority of the victims. An epidemic in New York in 1916 killed 2343 people and crippled many more. Efforts to keep people alive by mechanical means were similar to those in use now against Covid-19: the world’s first ICU unit was established to combat the polio epidemic in Copenhagen in 1952, with two hundred medical students recruited to pump oxygen and air manually into the lungs of patients who could no longer breathe on their own.
These epidemics were terrifying because people didn’t understand why children were falling ill when they hadn’t been in contact with any other sufferers. In reality, everybody was infected without knowing it. Various communities, usually immigrants, were scapegoated. In New York in 1916 animals were suspected of spreading the disease and 8000 dogs and 72,000 cats were killed. Many communities made ineffectual efforts to quarantine themselves: towns in Long Island and New Jersey sent out deputy sheriffs armed with shotguns to police the roads and turn back cars containing children under the age of 16. By the time of the Cork epidemic forty years later, doctors had come to understand the mechanism by which the virus found its victims but the knowledge wasn’t widely shared. My parents never grasped that the very isolation of Brook Lodge made it more dangerous than the worst slum housing in Cork.
In 1998 I went to Cork city and interviewed as many doctors, nurses and surviving victims as I could. The victims were easy to find – most of them, like me, had got the disease when they were small children. The medical staff who had treated them were harder to track down and many were no longer alive. I asked Kathleen O’Callaghan, who had treated me in St Finbarr’s, why there was so little published material about an event that had paralysed part of Ireland for a year. She said the reason was sheer terror: ‘People were that frightened at the time that they wanted to forget it. I would see people cross the road rather than walk past the walls of the fever hospital.’ The fear started to lift in 1954, when the American virologist Jonas Salk discovered an effective vaccine against polio. Two years later, while the epidemic was gripping Cork city, it was being used successfully to suppress an epidemic in Chicago. The vaccine did finally reach Ireland, in small quantities at first, with the most vulnerable age groups being vaccinated, though its availability was limited thanks to the theft of part of the first consignment.
I wasn’t sure how accurate my memories of Gurranabraher were and wondered whether others had had as bad a time in hospital as I had. I talked to Helena Casey, the daughter of a bus driver in Cork, who was one of the first victims of the epidemic. She recalled two nurses, one short, one tall. They were, she said, ‘real dragons. We all hated them. It was like prisoners against the Nazis.’ Her sister Pat, who was three at the time, had an even worse experience: like me a few months later, she stopped speaking. ‘I didn’t talk to anybody,’ Pat said. ‘I used to hide under the kitchen table when visitors came to the house because I thought they would take me back to the hospital.’
In 2005, having come to feel that I had learned as much about the epidemic as I ever would, I published a memoir, The Broken Boy. In the final chapter, I wrote that polio was probably the last in the line of diseases – cholera, typhus, malaria, yellow fever – capable of causing serious epidemics around the world. Polio epidemics had a surprisingly short career: less than seventy years between the end of natural immunity and the widespread use of the Salk vaccine. It was a story with a seemingly happy ending. Few people realised – certainly I didn’t – that if polio epidemics were a product of modernity then the way might be open for other epidemics of equal severity.
The behaviour of the coronavirus, when it surfaced in Wuhan at the end of last year, resembled that of the poliovirus in certain important respects: both are highly infectious and most of those infected have few if any symptoms and swiftly recover. But they become carriers all the same, infecting others, some of whom may belong to the unlucky 1 or 2 per cent – there is great dispute about the fatality rate among victims of Covid-19 – who will feel the virus’s full destructive impact. Methods of combating the two viruses are similar: when the queen visited Australia during a polio epidemic in 1954 there were fears that the crowds of schoolchildren assembling to greet her might pass the virus to one another and maybe even to the young monarch herself. So the Australian government launched a mass hand-washing campaign, leading to a drop in the number of children contracting polio during the royal visit. Nobody seemed embarrassed by the fact that no such effort had been made before the queen’s arrival prompted it.
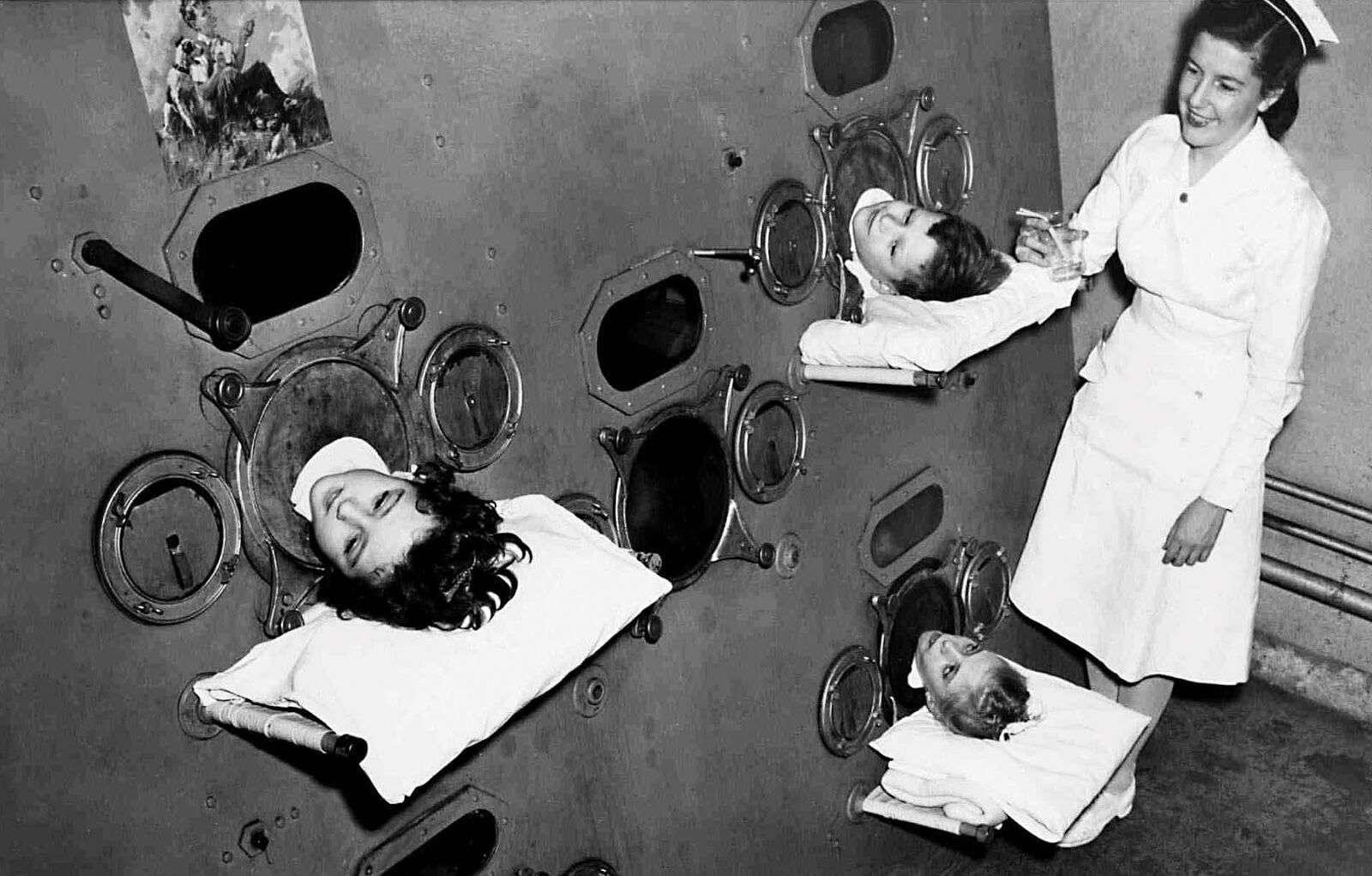
The poliovirus was worse for the very young; for the coronavirus it’s the old who are hardest hit. In both cases respiratory aids – the ‘iron lung’ and the ventilator – have been symbols of the struggle to keep people alive. In Cork in 1956, doctors didn’t seem to grasp how frightening such machines were for children: when I was in St Finbarr’s, one girl screamed and struggled when doctors tried to put her inside an iron lung because she thought it was an actual coffin and she was being buried alive. Politicians often compare the campaign to suppress the coronavirus to waging war against a dangerous enemy: they wrap the flag around themselves and call for national solidarity. Fear and a need to see visible action to counter it are a feature of all epidemics. In Cork, doctors were convinced that the disease would only be stopped when it ran out of victims. Jack Saunders, the city’s chief medical officer, insisted that a real quarantine was impossible because ‘for every case detected there were one or two hundred undetected or undiagnosed in the community, principally among the children.’ He opposed the cancelling of sporting fixtures and the closing of schools, a position echoed by the UK government’s chief medical officer, Chris Whitty, and chief scientific adviser, Patrick Vallance, in the early stages of the epidemic this year.
The city fathers in Cork were determined not to let their hotels and shops be ruined by the epidemic and largely succeeded in preventing damaging information getting out. They were helped by their influence over the Cork Examiner, the city’s main source of news. On 7 July 1957 it carried an article – not leading the front page – under the headline CORK CITY POLIO OUTBREAK: SIX CASES. The subheading added: NO OCCASiON FOR UNDUE ALARM – MEDICAL OFFICER. The paper gave daily updates on the number of new cases, but it usually led with news about the Suez Crisis or the Hungarian Uprising. Stories about polio were always followed by an upbeat subheadline such as PANIC REACTION WITHOUT JUSTIFICATION. My father later wrote that owners of major shops and businesses had threatened to withdraw their advertising from the Examiner unless the paper stopped reporting on the epidemic. When I looked through the archives, I found that there was almost no reporting of the epidemic after 12 September, two and a half weeks before my diagnosis.
I used to think that the efforts of the political and commercial elite in Cork to suppress the truth about the epidemic were unforgivable. But in the context of Covid-19 I can see that these local leaders had a point, even if they were motivated by self-interest alone. Coverage of the present pandemic has many of the failings of war reporting: it is sensationalist and melodramatic; the hunger for information and facts is so great that the most dubious data leads the news agenda. Figures for the numbers of Covid-19 cases merely reflect the number tested. Nobody knows whether the virus is the occasion or the cause of many of the deaths. The need of governments to show that they are taking action leads to panic and ill-advised policies – a feature of all epidemics, but especially this one. There are constant appeals in Britain to the resolution and unity of 1940, but the country is visibly closer to the chaos of 1914: incompetent and inexperienced leaders, shortages of essential equipment, enthusiastic but untrained volunteers – all leading to high numbers of casualties on the front line for little gain.
Send Letters To:
The Editor
London Review of Books,
28 Little Russell Street
London, WC1A 2HN
letters@lrb.co.uk
Please include name, address, and a telephone number.
